Reclaim Patient–Centered Care with Simple, Yet Smart, Medical Practice Technology
Deliver phenomenal patient and physician experiences with an integrated EHR, Practice Management, and Revenue Cycle Management (RCM) platform from OmniMD. We integrate EHR, Practice Management, and Revenue Cycle Software and Service into one solution to let you spend more time with patients, increase productivity, ensure information exchange, and improve your bottom line.



WE HAVE YOUR BACK FROM PATIENTS AND
PARTNERS TO FRONT OFFICE THROUGH BACK OFFICE

Patients
Improve the patient experience with an online portal, secure emails and text reminders and alerts, online scheduling and bill pay, and access to medical records.

Front Office
Schedule patients, verify insurance, collect copays, preauthorize, manage tasks, and sync with billing team.

Middle Office
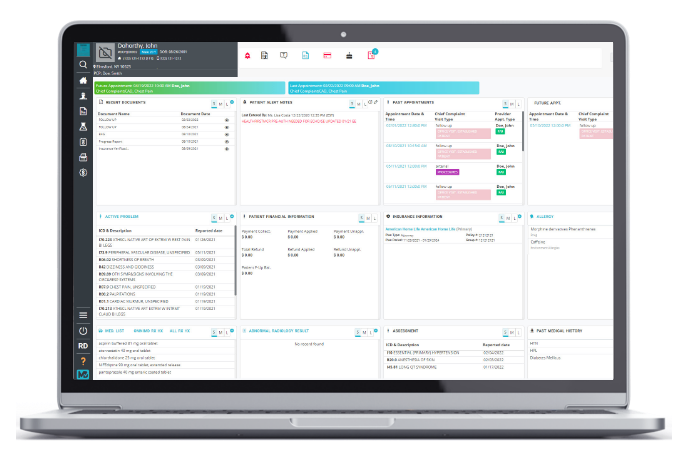
Intuitively Chart patient medical records, prescribe meds electronically, make informed decisions, generate benchmarks, and report on outcomes and measures.

Back Office
Manage coding, scrub claims, post co-pays and insurance payments, optimize process with integrated billing system and services to realize more revenue.

Partners
Connect and share data with ACOs, HIEs, medical billing companies, referring physicians, diagnostic laboratories, pharmacies, medical imaging, clinical associations and registries.
OUR FEATURES

EHR Software
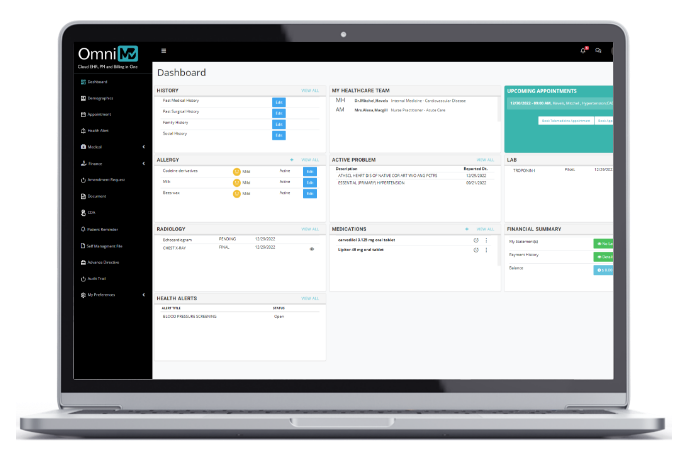
Simple yet savvy patient charting, decision-making, data transfer, and reporting.
Practice Management
Integrated practice management and billing software for better scheduling.

Patient Portal
Engage your patients with a wide variety of self-help tools and time-saving features.

Telehealth
Enable virtual visits to reduce travel and improve the patient experience.

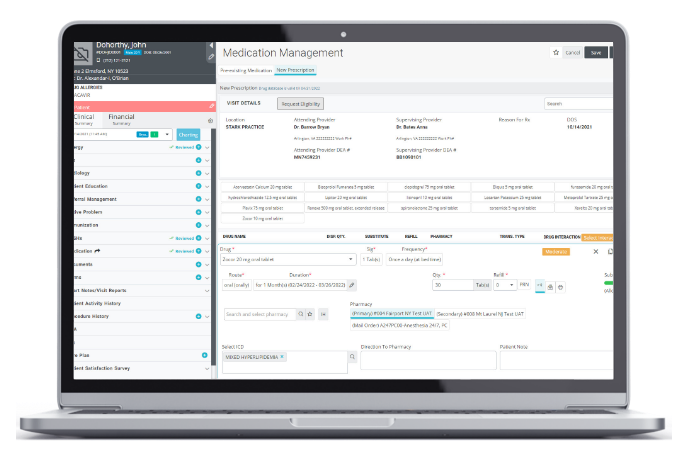
ePrescribing
Fast, safe, and securely prescribed controlled and non-controlled drugs.

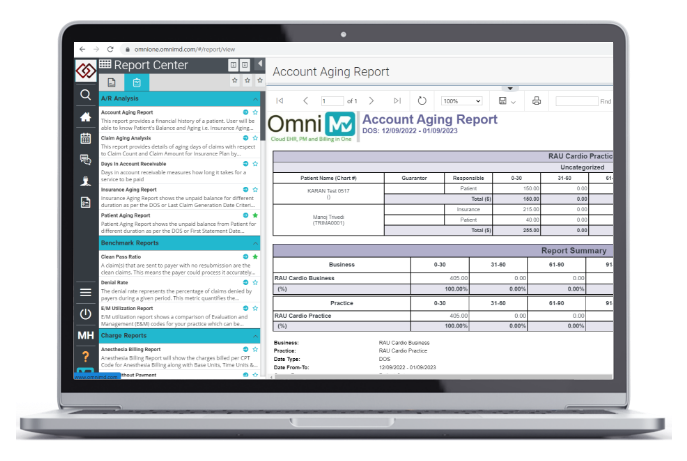
Managed Billing Services
Reduce staff and office footprint with outsourced revenue cycle management.



WHY CHOOSE OMNIMD
%
Healthcare Professionals
%
Healthcare Facilities
%
Customer Service Excellence
%
Patients Records
%
Uptime
%
Customer Retention
Connect with Us
Certificates

